Affordable overbite treatment in Melbourne.
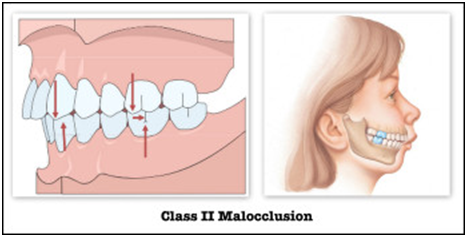
Class II problems- Increased Overbite.
Class II malocclusion problems occur when the upper jaw and teeth project ahead of the lower jaw.
A malocclusion is an imperfect bite, where ‘bite’ refers to the position of the teeth when the mouth is closed. In an ideal bite, the teeth close easily and lightly together in a zig-zag manner and make it easy to chew and maintain good oral hygiene.
Causes
- Class II problems can either be related to the size and position of one or both the jaws. Most jaw problems are inherited, and patients may either exhibit a smaller lower jaw (or mandible), bigger upper jaw (or maxilla) or a combination of both.
- When the Class II malocclusion is of a dental origin i.e. due to the incorrect position of teeth, it may be due to insufficient space for the teeth in the upper jaw or it may be associated with persistent habits like thumb sucking or finger sucking in children of school age. In both cases, the upper teeth usually tend to sit more forward and may appear more proclined (leaning forward).
- Other causes for a dental Class II problem may be early exfoliation of deciduous teeth or ectopic eruption of teeth (that is, if the baby teeth are lost early, or if teeth come through in irregular positions).
Clinical or facial features
Class II Division I
Most patients with Class II problems tend to show a more convex facial profile. They may have an increased overjet which leads to difficulty in closing their lips together, called lip incompetency. Their lower lip may get stuck behind their upper teeth, causing lip-biting problems.
Patients with a small lower jaw tend to have a small chin which may cause the upper teeth to appear too large, when in fact it is the lower jaw that causes the problem. However, in-class II patients where the upper jaw or teeth are sitting forward, the lower jaw may be of normal size. In this case, it is the upper jaw and the lip that are more pushed forward.
Patients with Class II dental problems may also have a mouth breathing tendency, either due to the position of their lips or protruded upper teeth, or a combination of these, combined with a narrower upper jaw particularly as a result of thumb or finger sucking habits.
When children suck their thumb, the thumb is placed behind the upper front teeth on the palate which pushes the upper front teeth forward. Also, as the child actively sucks the thumb with their lip and cheek muscles, these tend to push the side teeth inward, resulting in a v-shaped narrow upper jaw. The thumb position also causes the lower teeth to be pushed backward and may disrupt or inhibit the forward growth of the lower jaw, making the Class II problem worse. Since the thumb is placed between the upper and lower teeth it tends to leave an open bite as the front teeth are not able to overlap each other as they would in a normal bite.
Some children and adults who tend to have a smaller and more backward placed mandible (lower jaw) may also suffer from functional difficulties, including snoring, labored breathing, and lisping.
Class II Division II
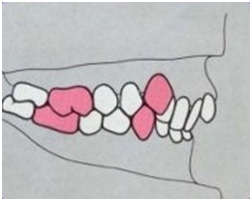
There is a however a type of class II malocclusion that is quite different from the above classical presentation which is characterized by the front two to four teeth being inclined inwards or backward (retroclined). These individuals most often tend to show a deep bite, where the upper teeth overlap the lower teeth more than normal causing injury to the gums on the palatal aspect of the upper teeth; the lower teeth are almost fully hidden behind the upper teeth on biting down and are not visible from the front. The deep bite may cause more wear and tear of the lower front teeth making them shorter in height over years and causing them to chip and break. This problem is called as a Class II division II malocclusion.
Treatment options
There are multiple treatment options for correction of the Class II malocclusion depending on the cause of the problem i.e. skeletal or dental, the severity of the problem, and the age of the patient.
Class II dental problem treatment options:
- Treatment of very mild dental class II problems may only require braces or clear aligners like Invisalign with elastics or rubber bands to correct the bite.
- In some cases where limited space gain is required (less than 5mm) for alignment of crooked teeth or pushing the upper teeth backward, this can be achieved either by arch or teeth expansion or by shaving of teeth called inter-proximal reduction (IPR) of mostly up to 0.5mm per tooth. The type of treatment required will mostly depend on the cause of the class II problem.
- For class II dental problems requiring more than six to eight millimeters of space, extractions may be needed. The teeth that are most commonly extracted include the first or the second premolars (i.e. teeth number four or five when counted from the front tooth backward on each side).
Class II skeletal or jaw treatment options:
- In growing patients, where the problem is due to the lower jaw being smaller, or in patients with a combination of a narrow upper jaw and small lower jaw, functional appliances may be used with an upper jaw expander to correct the jaw size. Most often the patients are generally reviewed for potential orthodontic treatment as early as seven to eight years of age. However, actual treatment may only be planned for later. The timing of treatment for children will vary as most jaw growth modulations are done according to the growth spurt of individual jaws.
- When an upper jaw expander is required to correct a V-shaped narrow arch, this is planned around the growth of the upper jaw. This may be done from seven to twelve years of age; however individual timing may vary from this.
- If the upper jaw needs to be restricted in growth as it growing at an accelerated growth, extraoral headgear may be used with either part braces or removable plates.
- The lower jaw can be modulated to improve the final jaw position when treatment is done with functional appliances like the Twin Block appliance, Herbst appliance, Twin Force Bite Corrector, Forsus appliances etc. The choice of appliance is on a case-by-case basis, with the goal of treatment being to try and encourage more jaw growth and forward position of the lower jaw. In most cases, some upper jaw expansion may be required with these bite corrector/jumper type appliances. This can be achieved with either a fixed upper arch expander or even with braces if only a mild expansion is required. The timing of treatment with the functional appliances must be in sync with the lower jaw growth which may be around the pre-pubertal age. The best way to assess this is to keep patients under review over their growing years to plan best timing to treatment.
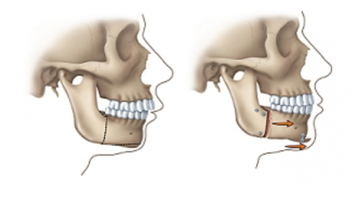
2- In non-growing patients or adults who have completed their growth, correction of the small lower jaw may require surgical correction called orthognathic surgery. This is done in tandem with braces. The patient sees their orthodontist along with a maxillo-facial surgeon who plans the position of teeth and jaws to achieve a stable Class I correction. Some patients may also require surgically assisted expansion of the upper arch followed by braces and then a second stage of lower jaw advancement surgery to correct the Class II skeletal problem.
3- Some adults who do not wish to undergo a surgical correction and have a mild to moderate skeletal Class II problem may be able to undergo camouflage treatment without surgery. This involves possible extraction of upper first or second premolars to move the teeth backward to hide the problem of a smaller lower jaw or an increased overjet and overbite.
As highlighted above, there are several treatment possibilities, which will be discussed with you at your free initial consultation and treatment options provided to customise your treatment plan to achieve the best possible result.
How Smile Avenue Specialist Orthodontists can help you
Free consultation
At Smile Avenue Orthodontics Melbourne, the first consultation is free for every new patient. This gives you the opportunity to talk with our doctors about your problem and to ask any questions you may have. Our doctors are experienced in providing different types of treatment and will outline a suggested treatment plan for you.
Experience and research in orthodontics
We use evidence-based methods, to ensure that we get the best outcome for you and your smile. This sets us apart from other orthodontic practices and means that we base all of our work on sound research and years of experience.
Our treating orthodontists have written numerous research publications in the field of complex orthodontics, which have been published in leading journals. Please click here to browse through our extensive body of research work.
Interest free payment plan
We offer affordable, no deposit and interest-free and low deposit flexible payment plans to all patients in. We also offer group discounts for families with more than one patient requiring treatment.
3D scanner
Our practice has the most recent digital scanner technology, that allows us to show you the results before treatment commences. We take a digital scan of your teeth and show you how your teeth will look at stages throughout your treatment and at the conclusion of your treatment. Patients find it comforting to see their treatment plan and result simulations before even starting the treatment.
FAQs
How long does the treatment take?
Treatment time depends on the type of treatment that may suit your clinical case and severity of the problem and. Treatment times may be as short as 12 months if it is only a mild class II dental problem. Most cases requiring extractions or jaw surgery may take 18-24 months for completion. The growing patients or adolescents where jaw growth modulation is planned may take up to 24-36 months over one or two phases of treatment to achieve the desired correction.
How much pain is involved?
With the introduction of new treatments and techniques, there is very little pain involved. Most patients describe their orthodontic work as causing ‘discomfort’ rather than ‘pain’.
Most patients undergoing surgical correction and treatment are concerned about the pain associated with the procedure. However, with recent advances in surgical techniques the pain following surgical procedures has minimised. Most patients stay in the hospital for post-operative care for only three to four days. All patients are reviewed by their maxillofacial surgeons a week after discharge from hospital to ensure patient wellbeing and provide a prescription for pain relief as per individual case basis.
What are the treatment costs?
For information regarding braces costs, please click here.
What after-treatment care will I need?
All patients who undergo orthodontic work require some type of retainer, to ensure that the teeth do not revert to their original position. There are several choices of retainers, each with its own advantages and disadvantages:
- A lingual retainer (‘lingual’ means ‘related to the tongue’; this retainer is behind the teeth, near the tongue). A lingual retainer is permanently fixed to the back of the teeth. It is invisible, and although some patients report that it ‘worries’ their tongue, most eventually become used to it.
- A clear removable plastic retainer (Essix type). This type of retainer is very popular as it is not visible, is comfortable, and doesn’t cover the palate. However, it is relatively fragile, and has an average life expectancy of about one to two years, depending on whether the patient grinds their teeth and how well they look after it.
- A plate type of removable retainer e.g. Hawley retainer (a ‘traditional retainer’). This type of retainer is much sturdier than a clear retainer, but as it covers the palate, some patients find it more difficult to tolerate. Also, it has a metal wire that runs across the surface of the front teeth and is more visible than the clear alternative.
How long will I need to wear a retainer?
Retainers are essential in preventing the teeth from moving back to their original pre-treatment condition. Most health funds will pay for orthodontic work only once in a patient’s life, so for most patients, this is a once-in-a-lifetime opportunity. Because of this, it is good to view a retainer as ‘for life’.
- A lingual retainer is permanent and can be left there for life.
- Removable retainers (e.g. clear Essix and Hawley) need to be worn full time for first 3 to 6 months, then the time may be able to be gradually reduced, but this depends on the individual case.
Free initial consultation, provided to all new patients . For information regarding braces costs please click here.